I have discovered that the
medication nalmefene (Selincro®)
has the potential to treat all symptoms of
Post-traumatic Stress Disorder in 2-3 weeks.
I have discovered that the medication nalmefene (Selincro®)
has the potential to treat
all symptoms of
Post-traumatic Stress
Disorder in 2-3 weeks.
Hillel Glover, M.D.
Hillel Glover, M.D.

About Hillel Glover, M.D.
I am a psychiatrist who specializes in the study and treatment of Post-Traumatic Stress Disorder (PTSD).
When working with Vietnam combat veterans, I saw firsthand how devastating the effects of trauma are
and how disabling this condition can be. I became profoundly aware of emotional numbing being a major
stumbling block in treating people with PTSD. This led me to discover that a specific type of opioid
antagonist (opioid blocker) could successfully treat emotional numbing.
I am a psychiatrist who specializes in the study and treatment of Post-Traumatic Stress Disorder (PTSD). When working with Vietnam combat veterans, I saw firsthand how devastating the effects of trauma are and how disabling this condition can be.
My Professional Training
University of Miami
Miller School of Medicine, M.D.
Brooklyn V.A. Hospital
Internship
Hillside Hospital
Queens, NY – now part of Long Island Jewish Hospital
Adult Psychiatry Residency
State University of New York
Downstate Medical Center
Research Post Graduate Fellowship
New York Medical College
Psychoanalytic Training Institute
Columbia Presbyterian Hospital, New York
Child Psychiatry Residency
Teaching
Maimonides Medical Center,
Director of Child Psychiatry
Dartmouth Medical School,
Assistant Professor
Certification and licenses
- Board Certified in Psychiatry
- Board Certified in Child Psychiatry
- Certified in Psychoanalysis
- Board Certified Expert in Traumatic Stress
Awards
- Citation of Meritorious and Conspicuous Service Military Order of the Purple Heart
- Chapel of Four Chaplains Legion of Honor
An Accelerated Method

I originally hypothesized that the opioid antagonist nalmefene, marketed in Europe and Israel as Selincro®, would reverse the numbing/deadness that people with PTSD experience. I conducted a one year 11 month open label pilot study using this drug to treat Vietnam combat veterans and one World War II veteran, results of which are published in the Israel Journal of Psychiatry.
Much to my amazement, nalmefene did so much more than I expected; it was serendipitous that it significantly reduced or remitted all symptoms of PTSD. Based on these findings, I conclude that the endogenous opioid system mediates the expression of all symptoms of PTSD. I believe the key to pharmacologic treatment of emotional numbing is the same key that unlocks the treatment for PTSD. This lead me to receive a patent, Method for treating post-traumatic stress disorder, in the U.S. (2021), Israel (2023), and the EU (2024). This patent is based on an accellerated dose titration method, which enables patients to reach an optimal dose in 2-3 weeks.
“I believe the key to pharmacologic treatment of
emotional numbing is the same key that unlocks the
treatment for all symptoms of PTSD.”
“I believe the key to pharmacologic treatment of emotional numbing is the same key that unlocks the treatment for all symptoms of PTSD.”
The German Study
In 2021, Dr. Frank Enning, Vice Chairman of the Department of Psychosomatic Medicine and Psychotherapy, Central Institute for Mental Health, Mannheim, Germany, and Dr. Christian Schmahl, Medical Director of the Clinic for Psychosomatic and Psychotheraputic Medicine, Central Institute for Mental Health and Professor of Psychosomatics and Psychotheraputic Medicine at Heidelberg University, conducted a study in which patients diagnosed with borderline personality disorder and complex PTSD were administered nalmefene. Thirteen out of the 17 patients showed a significant reduction in dissociative phenomena during the course of treatment. It is important to note that Complex PTSD is associated with depression, anxiety, aggression and violence, drug abuse, dissociation, paranoia, and suicide.
A 22 year old patient who was diagnosed with Borderline Personality Disorder and complex PTSD was abused physically and sexually on a regular basis from the ages of 4 to 18 by her father. She suffered from daily dissociative seizures, which significantly diminished in frequency, intensity, and duration when she was administered higher doses of nalmefene. She also experienced severe mood swings, feelings of emptiness, suicidal ideation, self-harm by scalding, intrusive thoughts, and nightmares. In an email correspondence with Dr. Schmahl on December 2, 2024, he stated that he observed a clinical reduction of all of these symptoms in response to nalmefene.
It is important to note that patients in the Enning-Schmahl study only received 162 mg nalmefene once a day as the maximum available dose, rather than 200 mg twice a day in the study I conducted. Also, four patients had to be discontinued at a starting dose of 18 mg per day, and another patient at a starting dose of 36 mg per day. The accelerated method in my patent recommends a starting dose of 50 mg twice a day, which bypasses the opioid withdrawal symptoms that are observed at lower doses.
Results of the study, Treatment of dissociative symptoms with nalmefene in patients with borderline personality disorder and complex posttraumatic stress disorder, were published in Der Nervenarzt, 2021.
The Nalmefene Pilot Study
The Nalmefene
Pilot Study
Between 1988-1990, I administered the opioid antagonist nalmefene to Vietnam combat veterans and one WWII veteran, all of whom were diagnosed with PTSD. The eight veterans who went to the highest dose of 200 milligrams twice a day reported that all of their symptoms of PTSD significantly improved or went into remission. My original hypothesis was that the drug would reverse the numbing response. The fact that all symptoms of PTSD (including nightmares, flashbacks, intrusive thoughts, emotional numbing and avoidance, feelings of detachment and estrangement from others, psychological and physiological reactions to reminders of trauma, hypervigilance, hyperarousal, exaggerated startle response, disturbed concentration and memory, angry outbursts and aggressive behaviors, irritability, feelings of vulnerability, mistrust of others, and dissociative symptoms, including amnesia) were remitted or significantly reduced led me to believe that the endogenous opioid system modulates the expression of traumatic symptoms.
I believe that one important way the endogenous opioid system does this is through specifically stimulating the kappa opioid receptor system. Stimulation of the kappa opioid receptors has been identified in experimental literature as being associated with inducing dysphoric mood states. This same receptor system is also associated with problems relating to stress, trauma and addictions. By contrast, the mu opioid receptor system is associated with pleasure and reward. I firmly believe the dysphoric mood state associated with stimulation of the kappa opioid receptor system is associated with the experience of being numb.
At higher doses of nalmefene (100 milligrams twice a day and above), the veterans felt increasingly more emotionally stable, self-confident, and were able to spontaneously discuss their combat experiences without any psychophysiological distress. They no longer felt as vulnerable as they did at doses below 100 mg twice a day.
It is my hope that more studies will be initiated with nalmefene for the treatment of PTSD using standardized measures of PTSD, including the Glover Vulnerability Scale (GVS)© and the revised Glover Numbing Scale©.
I am grateful to Elliot Hahn, Ph.D., a dear friend and brilliant mentor who was an inventor of nalmefene. He served as Senior Vice President of Research at IVAX Corporation, which provided me with nalmefene when I conducted my 23 month pilot study. May his memory always be a blessing.
It is my hope that more studies will be
initiated with nalmefene for the treatment
of PTSD using standardized measures of
PTSD, including the Glover Vulnerabilty
Scale (GCS)© and the revised Glover
Numbling Scale (GNS-R)©.
PTSD RESEARCH & DATA | 2025–2026
The Global Burden of PTSD
The Global
Burden of PTSD
Prevalence, economic impact, and intergenerational consequences across the
US, EU, Japan, and the Middle East.
PTSD Prevalence
economic burden — US alone
experience a traumatic event
populations
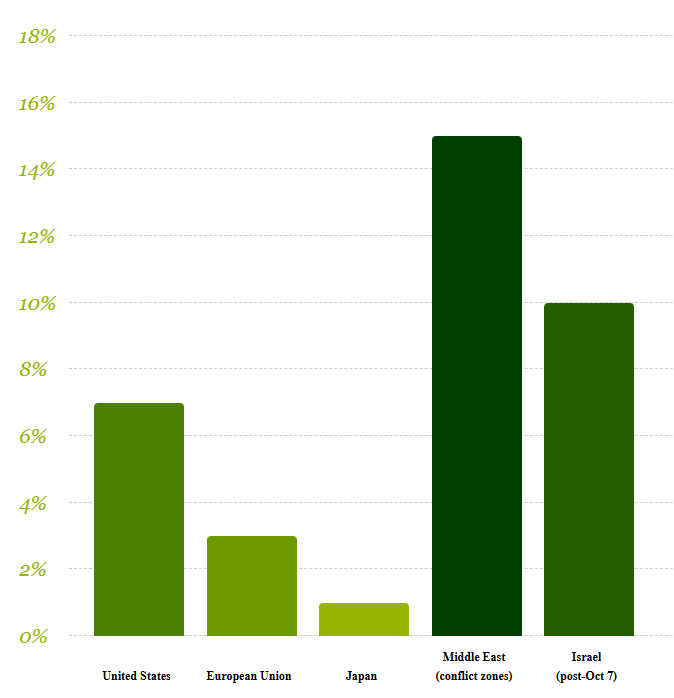
PTSD Prevalence Across Regions
PTSD Prevalence
Across Regions
Lifetime prevalence (%) by region — current data 2025
(conflict zones)
(post-Oct 7)
US Breakdown
Lifetime vs annual rates
Lifetime prevalence
General population
Annual prevalence
~13 million Americans/year
Veterans (lifetime)
Varies by conflict era
Women vs men
Women twice as likely
Source: NIMH; VA National Center for PTSD (2024)
Regional Context
Where rates are highest globally
Japan
Among lowest globally; cultural stigma
+ low trauma exposure
Japan
Among lowest globally; cultural stigma + low trauma exposure
EU average
Higher in Eastern Europe;
rising post-COVID
EU average
Higher in Eastern Europe; rising post-COVID
Israel (post-Oct 7)
10% PTSD; 60%+ PTS
symptoms (ICAR 2025)
Israel (post-Oct 7)
10% PTSD; 60%+ PTS symptoms (ICAR 2025)
Conflict zones
WHO: 3× higher in war-exposed
populations
Conflict zones
WHO: 3× higher in war-exposed populations
Source: NIMH; VA National Center for PTSD (2024)
All data sourced from peer-reviewed research and official government/institutional
reports. Where regional comparisons span different time points, this is noted in chart
annotations. This dashboard is intended for educational and advocacy purposes.
Data compiled 2025–2026
Primary sources: WHO, NIMH, VA, ICAR,
PMC/PubMed
According to the World Health Organization (WHO), as of 2025, approximately 3.9% of the world’s population – about 321 million people - have experienced PTSD at some point in their lives. Common causes of PTSD include combat military service or exposure to war, childhood abuse, violent assaults, sexual violence, severe accidents, natural disasters, witnessing a traumatic event, life-threatening situations, or a long-term illness (medical PTSD). Ongoing, repeated trauma that is inescapable can result in Complex PTSD (CPTSD).
All data sourced from peer-reviewed research and official government/institutional reports. Where regional comparisons span different time points, this is noted in chart annotations. This dashboard is intended for educational and advocacy purposes.
Data compiled 2025–2026
Primary sources: WHO, NIMH, VA, ICAR,
PMC/PubMed
According to the World Health Organization (WHO), as of 2025, approximately 3.9% of the world’s population – about 321 million people - have experienced
PTSD at some point in their lives. Common causes of PTSD include combat military service or exposure to war, childhood abuse, violent assaults, sexual
violence, severe accidents, natural disasters, witnessing a traumatic event, life-threatening situations, or a long-term illness (medical PTSD). Ongoing, repeated
trauma that is inescapable can result in Complex PTSD (CPTSD).
According to the World Health Organization (WHO), as of 2025, approximately 3.9% of the world’s population – about 321 million people - have experienced PTSD at some point in their lives. Common causes of PTSD include combat military service or exposure to war, childhood abuse, violent assaults, sexual violence, severe accidents, natural disasters, witnessing a traumatic event, life-threatening situations, or a long-term illness (medical PTSD). Ongoing, repeated trauma that is inescapable can result in Complex PTSD (CPTSD).
Founded by Dr. Hillel Glover, PTSD Global, LLC is devoted to developing and promoting novel accelerated treatments using the opioid antagonist nalmefene (Selincro) for the research and treatment of Post-traumatic stress disorder.
Press
Press — A combat
Vietnam medic's
transformation on
Nalmefene
Click THUMBNAIL to enlarge
Press — A combat
Vietnam medic's
transformation on
Nalmefene
Press — A combat
Vietnam medic's
transformation on
Nalmefene
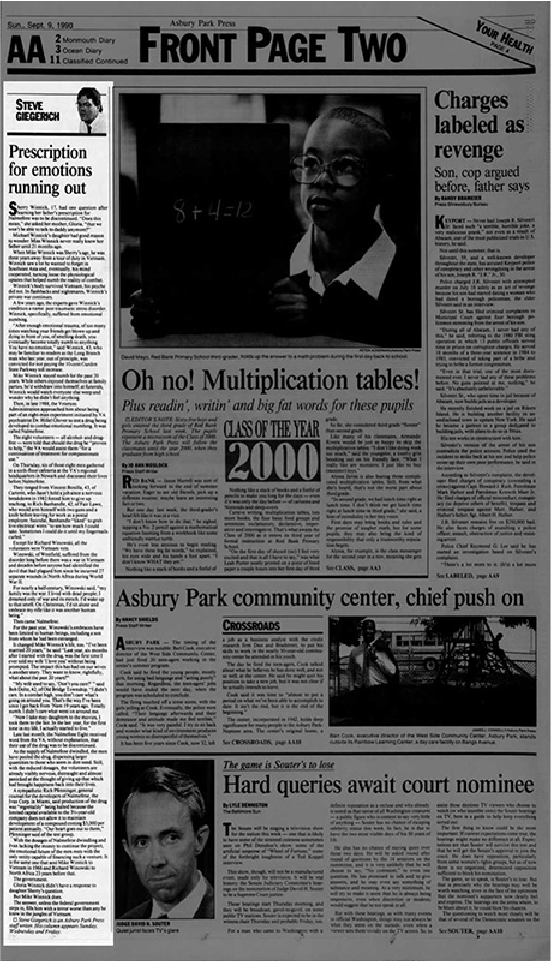
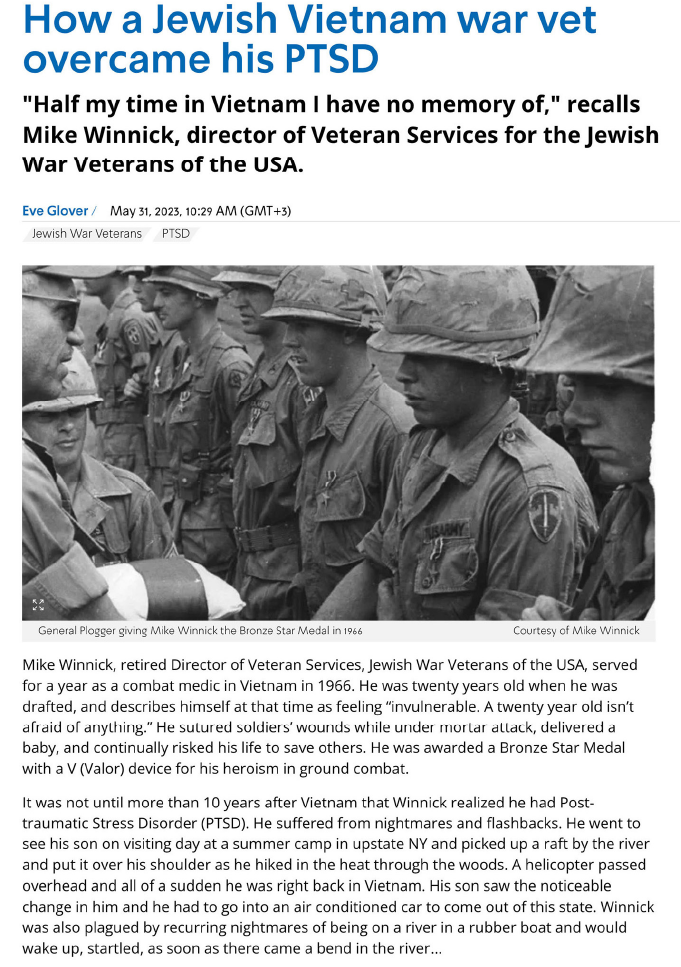
The Asbury Park Press article, “Prescription for emotions running out,” was published after the study ended
and veterans were hanging on to the remaining amount of nalmefene they still had. It relays how nalmefene
dramatically changed their lives. Mike Winnick, a Vietnam combat medic and retired Director of Veteran
Services, Jewish War Veterans of the USA, was interviewed again in 2023 for an Israel National News article,
“How a Jewish Vietnam war vet overcame his PTSD.” Winnick reported that he continued to receive positive
benefits from nalmefene for twenty-three years after the drug study ended.
The Asbury Park Press article, “Prescription for emotions running out,” was published after the study ended and veterans were hanging on to the remaining amount of nalmefene they still had. It relays how nalmefene dramatically changed their lives. Mike Winnick, a Vietnam combat medic and retired Director of Veteran Services, Jewish War Veterans of the USA, was interviewed again in 2023 for an Israel National News article, “How a Jewish Vietnam war vet overcame his PTSD.” Winnick reported that he continued to receive positive benefits from nalmefene for twenty-three years after the drug study ended.
Dramatic Life Changes
in Veterans on Nalmefene
I was limited in terms of how much observational information I could include in my
report because this was a pilot study, and I was allotted a finite amount of space in
the journal. All eight of the veterans who went up to the maximum available dosage
of nalmefene (200 mg twice a day) went into remission or experienced significant
improvement in all symptoms of PTSD. Below is a description of the dramatic
changes in the lives of five of these eight veterans.
I was limited in terms of how much observational information I could include in my report because this was a pilot study, and I was allotted a finite amount of space in the journal. All eight of the veterans who went up to the maximum available dosage of nalmefene (200 mg twice a day) went into remission or experienced significant improvement in all symptoms of PTSD. Below is a description of the dramatic changes in the lives of five of these eight veterans.

1. As the dosage of nalmefene increased above 100 milligrams twice a day, all of the veterans
improved correspondingly in profound ways. The “wall” that stood between them and other people
changed as a visual entity in its solidity, texture and height. Some veterans described this wall as first
appearing like thick, porous steel, then transforming into brick and becoming a shorter wall of thin
glass before finally disappearing. The “wall” had provided the veterans with the illusion of safety. It
changed and then disappeared as the veterans felt safer and less vulnerable in their environments.
1. As the dosage of nalmefene increased above 100 milligrams twice a day, all of the veterans improved correspondingly in profound ways. The “wall” that stood between them and other people changed as a visual entity in its solidity, texture and height. Some veterans described this wall as first appearing like thick, porous steel, then transforming into brick and becoming a shorter wall of thin glass before finally disappearing. The “wall” had provided the veterans with the illusion of safety. It changed and then disappeared as the veterans felt safer and less vulnerable in their environments.
1. As the dosage of nalmefene increased above 100 milligrams twice a day, all of the veterans improved correspondingly in profound ways. The “wall” that stood between them and other people changed as a visual entity in its solidity, texture and height. Some veterans described this wall as first appearing like thick, porous steel, then transforming into brick and becoming a shorter wall of thin glass before finally disappearing. The “wall” had provided the veterans with the illusion of safety. It changed and then disappeared as the veterans felt safer and less vulnerable in their environments.
2. All of their senses improved. Before the administration of nalmefene, the veterans described living in a world of grey with little sense of color or visual clarity. It was like living in a fog. Textures and tastes were also muted. Food frequently tasted like cardboard, and people could also appear as two dimensional silhouettes.
2. All of their senses improved. Before the
administration of nalmefene, the veterans described
living in a world of grey with little sense of color or
visual clarity. It was like living in a fog. Textures and
tastes were also muted. Food frequently tasted like
cardboard, and people could also appear as two
dimensional silhouettes.
2. All of their senses improved. Before the administration of nalmefene, the veterans described living in a world of grey with little sense of color or visual clarity. It was like living in a fog. Textures and tastes were also muted. Food frequently tasted like cardboard, and people could also appear as two dimensional silhouettes.

3. Two veterans spontaneously reported
experiencing loss of all drug cravings; one for
alcohol, and the other for cocaine.
3. Two veterans spontaneously reported experiencing loss of all drug cravings; one for alcohol, and the other for cocaine.
4. The veterans became increasingly self-aware as they broke out of the robotic state they had been trapped in. They felt and visibly appeared more alive and unconstrained.
It is important to note that the veterans who were on a dosage of nalmefene 200 milligrams twice a day became able to access a wide range of normal human emotions and feelings. They also no longer exhibited bouts of explosive rages, episodes of destructive anger, sadistic behaviors and consuming thoughts of plotting revenge. One veteran was preoccupied with fantasies of mounting a tower on a university campus and randomly shooting people. His flat affect and expressionless face became gleeful, and his mood euphoric, accompanied by sadistic laughter when relaying his fantasy.
This behavior completely stopped in
response to
nalmefene. He also began to
express genuine feelings of interest and
love towards his wife and son.
This behavior completely stopped in response to nalmefene. He also began to express genuine feelings of interest and love towards his wife and son.

4. The veterans became increasingly self-aware as they broke out of the robotic state they had been trapped in. They felt and visibly appeared more alive and unconstrained.
It is important to note that the veterans who were on a dosage of nalmefene 200 milligrams twice a day became able to access a wide range of normal human emotions and feelings. They also no longer exhibited bouts of explosive rages, episodes of destructive anger, sadistic behaviors and consuming thoughts of plotting revenge. One veteran was preoccupied with fantasies of mounting a tower on a university campus and randomly shooting people. His flat affect and expressionless face became gleeful, and his mood euphoric, accompanied by sadistic laughter when relaying his fantasy.
This behavior completely stopped in
response to
nalmefene. He also began to
express genuine feelings of interest and
love towards his wife and son.
This behavior completely stopped in esponse to nalmefene. He also began to express genuine feelings of interest and love towards his wife and son.
Numbing and Vulnerability are
Critical to Understanding Chronic PTSD
Numbing and Vulnerability are Critical to Understanding Chronic PTSD
I emphatically disagree with the decision to remove the term “numbing “ from the diagnosis of PTSD in the
DSM-5 (American Psychiatric Association, 2013). Numbing is the most common symptom of dissociation,
which includes having flashbacks, and experiencing derealization, depersonalization, amnesia and fugue
states. The phenomenon of numbing was much studied, examined and discussed within the field of PTSD
prior to the publication of the DSM-5. Some combat veterans were referred to as being the “walking dead.”
Robert J. Lifton’s groundbreaking book, Home from the War, was based on his work with reuniting Vietnam combat veterans. Lifton introduced the term “numbing” (p.45) and “psychic numbing” (p.278). Lifton described how combat veterans “underwent a gradual but profound process of numbing reflected in their increasing callousness and brutality toward Vietnamese.” In group meetings with Lifton, the veterans frequently referred to their difficulties in experiencing any kind of genuine feelings, reported feeling robotic (p. 274), or they pretended to have feelings they didn’t really have (p.276). Lifton also described how a veteran’s numbing had served to distance himself from feelings of guilt (p. 395)
I emphatically disagree with the decision to remove the term “numbing “ from the diagnosis of PTSD in the DSM-5 (American Psychiatric Association, 2013). Numbing is the most common symptom of dissociation, which includes having flashbacks, and experiencing derealization, depersonalization, amnesia and fugue states. The phenomenon of numbing was much studied, examined and discussed within the field of PTSD prior to the publication of the DSM-5. Some combat veterans were referred to as being the “walking dead.”
Robert J. Lifton's groundbreaking book, Home from the War, was based on his work with reuniting Vietnam combat veterans. Lifton introduced the term "numbing" (p.45) and "psychic numbing" (p.278). Lifton described how combat veterans "underwent a gradual but profound process of numbing reflected in their increasing callousness and brutality toward Vietnamese.” In group meetings with Lifton, the veterans frequently referred to their difficulties in experiencing any kind of genuine feelings, reported feeling robotic (p. 274), or they pretended to have feelings they didn't really have (p.276). Lifton also described how a veteran's numbing had served to distance himself from feelings of guilt (p. 395)
Glover Numbing Scale (GNS)©
What does it mean when a person says he/she feels numb? Feeling numb indicates that a person lacks access to or is disconnected from emotions such as happiness or joy, and cannot feel love, care and concern or intimacy with others. When feeling numb, a person also cannot experience feelings of sadness, depression, guilt, low self-esteem, suicide or self-hatred. It should be apparent that a numb state does protect a person from feeling depressed. People who feel emotionally numb invariably report that they would prefer to be numb than depressed. Similarly, the numb state protects a person from feeling embarrassed or ashamed.
One frequent source of confusion for clinicians regarding the phenomenon of numbness includes the fact that patients often mistakenly report symptoms of depression occurring at the same time as feeling numb. The vast majority of individuals who are numb do not stay in that mood state all the time – they typically switch between feeling numb and feeling depressed, but they are not in both states simultaneously. Symptoms synonymous with numbing include feeling hollow, dead, shut down and empty-no feelings .
The term “dead” denotes a more profound state of emotional withdrawal and lack of relatedness to others. Individuals who feel dead may complain of difficulty falling asleep because lying still intensifies the feeling of “deadness.” These individuals may value being in a state of movement when alert. Numb individuals may self-medicate with street opioids such as heroin in order to feel energetic and active, which can lead to addiction to opioids. Interestingly, drugs such as heroin can have the opposite effect on people who are numb.
Individuals who feel profoundly hollow have reported to me that they experience their bodies as being transparent, and feel as though others can literally see through them. They also reported believing they could walk through walls because their bodies have no physical substance.
Numbing, just like depression, can manifest as a circumscribed complaint or as a syndrome with an array of associated symptoms. Both depression and numbing can be associated with a loss of interest, pleasure, motivation, apathy, impaired concentration and memory, mental fog and fatigue. A person who is numb will not, however, experience the other symptoms unique to depression such as loss of self-esteem, sadness, guilt and suicidal ideation. I have only encountered one individual who was suicidal while in a numb state. This person became suicidal and was consequentially hospitalized because she could not tolerate her inability to experience normal human feelings.
Depressed people are invariably troubled and preoccupied by memories and events that occurred in the past, whereas people who are numb are very present oriented and not concerned with the past or the future, unless they are consumed by anger and thoughts of vengeance and revenge for past perceived grievances. In a numb state, a person may only be able to experience intense emotions such as anger and rage. I became acutely aware of this while treating a Vietnam veteran who had completed three tours of duty and was persistently numb. While attending a funeral of a loved one, he exploded into a rage in front of others who were mourning. Rage was the only emotion he was able to access. When people who are numb go into a rage, the event is especially intense, explosive and long lasting. While in a state of rage, people can lose all feelings of care and concern for others and for the consequences of their behavior. Afterward, they typically become withdrawn and unresponsive for a protracted period of time. Oftentimes they experience amnesia and cannot recall the event. Others recall seeing the color red in the center of their tunnel vision during their rage.
There are also other profoundly numb people who are unable to access feelings of destructive anger and rage. They are completely unresponsive, like a rock; they have a flat affect and no facial expressions, their speech is monotonic. Many chronically numb individuals learn to pretend to have feelings which they do not truly experience. Others are unaware that they are projecting facial expressions, such as anger or sadness, that are disconnected from and do not accurately reflect the numb state they are in.
Cognitive impairments in people who are numb tend to be more severe than in depressed individuals. For example, a numb person may experience mental blankness, periods of amnesia, and loss of self-awareness and the ability to monitor his/her own behaviors. In the case of people who report having severe depression, it is crucial for a clinician to make certain that the person is truly depressed and not numb.
Antidepressants are not effective in treating numbness. Somatic symptoms are also different in people who are numb verses people who are depressed. For example, people who are numb may experience analgesia (loss of bodily sensations), pins and needles and transient periods of paralysis while awake. It is not unusual for people who are emotionally numb to feel disconnected from their own identities and to wonder who they are because they feel so detached from themselves.
Numb people may adapt to feeling disconnected by creating an image for themselves that is associated with a strong visual identity such as “fashion queen” or “combat warrior.” If a person who is numb is not cognitively impaired in terms of his/her concentration and memory, this person may be able to function well in a business environment that does not require relating to others empathically. These individuals may function well in the workplace but very poorly in a family environment.
What kind of situations may precipitate the numb response? First and foremost is exposure to serious injury or possible loss of life. Overwhelming stress in some individuals such as loss of income, divorce, or death of a family member may precipitate an acute numb response rather than depression. Chronic unremitting depression or physical illness may ultimately lead to a numb response. Numbing resulting from exposure to trauma is more likely to be a conditioned (automatic) response, which predisposes that person to becoming numb in reaction to future stressors. Numbness becomes the predominant mode of response. Individuals who are chronically numb may experience waves of numbness that appear to come out of the blue. In these cases, the numb response appears to take on a rhythm of its own which seems at times to be independent of any identifiable stressor.
Dreams can vividly portray the mental state of the dreamer. One World War II veteran dreamt that he saw himself in the passenger seat of a space capsule constantly orbiting the earth. What a powerful way of illustrating the veteran’s sense of isolation and emotional distance from others. Interestingly, somatic analgesia and paralysis are two responses that can be found in lab rats and mice when they are exposed to stressful situations. Somatic analgesia is referred to as stress induced analgesia, when, for example, a laboratory animal’s foot is exposed to an electric shock while inside of a cage. Once conditioned, merely placing the animal in the same cage will induce analgesia, even in the absence of being shocked.
Studies of stress induced analgesia gave me the first important clue as to what was causing emotional numbing in humans. First I reasoned that the body and mind are one. Therefore, what was causing numbing or analgesia of the body could also be causing emotional numbing centrally. I learned there are four different neurochemicals that can be associated with stress induced analgesia, but only endogenous opioids can induce a conditioned form of stress induced analgesia. This was an important step in my realization that numbing (both somatic and central) has to be mediated by the endogenous opioid system. Not all people who are emotionally numb also have somatic analgesia, but in people who have both phenomena, invariably it is the somatic analgesia that appears first. Thus, a milder stressor is likely to induce somatic analgesia first without necessarily also inducing emotional numbing.
A very large study of 14,465 children and adolescents who were exposed to an earthquake in China in 2008 were assessed for their emotional numbing responses to this natural disaster. Participants who reported feeling numb in response to both positive and negative emotions had the highest risk for developing PTSD, most severe PTSD symptoms and functional impairments, with large effect sizes when compared with participants with no emotional numbing symptoms. Reporting only numbing of positive emotions had moderate effects, and reporting only numbing of negative emotions had smaller effects. The authors concluded that the results revealed associations between emotional numbing patterns, posttraumatic stress symptoms and impairments in quality of life (Li, G., Wang, et al (2020) An Item-Based analysis of PTSD Emotional Numbing Symptoms in Disaster-Exposed Children and Adolescents. Journal of Abnormal Child Psychiatry 48(10): 1303-1311).
Application of the Glover Numbing Scale (GNS)©
The GNS is a 35 item self-report scale that assesses the frequency of numb responses (emotional, somatic, cognitive, identity) for the past week. GNS scores significantly discriminated levels of numbing found in veterans in different Vietnam veteran facilities (in-patient veterans had the highest score on the GNS, out-patient veterans had a moderate score and veterans in veteran outreach centers had lower scores). Non-combat Vietnam vets had the lowest scores of all four groups.
Another study reported that women hospitalized with the diagnosis of either Dissociative Identity Disorder (DID) or the repetitive behavior of Self-Injurious Behavior (SIB) scored significantly higher on the GNS than women hospitalized with the diagnosis of Major Depressive Disorder (MDD). Therefore, the GNS distinguished women exposed to trauma (the first two groups mentioned above) from women with the diagnosis of MDD.
Furthermore, both the inpatient female MDD population and an outpatient male MDD population showed a bimodal distribution of scores on the GNS with a significant difference between the two subgroups of each population. Both the females and the males who scored significantly higher had histories of exposure to trauma.
The Beck Depression Inventory (BDI) had also been administered to the women. The BDI did not distinguish between the two subgroups with MDD in contrast to findings using the GNS. This result highlights the importance of using the GNS in people with the diagnosis of MDD in order not to confuse symptoms of numbing with depression.
The 2019 Revised GNS is a 35 item self-report scale with some additional information concerning the subjective state of the numb response.
The GNS is a 35 item self-report scale that assesses the frequency of numb responses (emotional, somatic, cognitive, identity) for the past week. GNS scores significantly discriminated levels of numbing found in veterans in different Vietnam veteran facilities (in-patient veterans had the highest score on the GNS, out-patient veterans had a moderate score and veterans in veteran outreach centers had lower scores). Non-combat Vietnam vets had the lowest scores of all four groups.
Another study reported that women hospitalized with the diagnosis of either Dissociative Identity Disorder (DID) or the repetitive behavior of Self-Injurious Behavior (SIB) scored significantly higher on the GNS than women hospitalized with the diagnosis of Major Depressive Disorder (MDD). Therefore, the GNS distinguished women exposed to trauma (the first two groups mentioned above) from women with the diagnosis of MDD.
Furthermore, both the inpatient female MDD population and an outpatient male MDD population showed a bimodal distribution of scores on the GNS with a significant difference between the two subgroups of each population. Both the females and the males who scored significantly higher had histories of exposure to trauma.
The Beck Depression Inventory (BDI) had also been administered to the women. The BDI did not distinguish between the two subgroups with MDD in contrast to findings using the GNS. This result highlights the importance of using the GNS in people with the diagnosis of MDD in order not to confuse symptoms of numbing with depression.
The 2019 Revised GNS is a 35 item self-report scale with some additional information concerning the subjective state of the numb response.
Glover Vulnerability Scale (GVS)©
Vulnerability has been reported to be a significant problem for Vietnam veterans suffering from PTSD. Behavioral science literature has highlighted the important fact that vulnerability is closely associated with mistrust and paranoid ideations. The GVS represents my effort to operationalize the construct of vulnerability based on information found in this literature, coupled with my own clinical observations.
Dr. Robert J. Lifton and Eric Olsen reported that the survivor of trauma was likely to experience a shattering of his or her illusion of invulnerability in "The human meaning of total disaster, the Buffalo Creek experience," Psychiatry vol. 39:1-18, 1976.
Lifton connected a veteran's dream of being naked to his experience of vulnerability associated with shame and guilt in his book, Home from the War, (p. 182). He also extensively addressed veterans' pervasive mistrust and fear of forming human relationships, which they desperately craved (p. 268). Lifton reported that a high number of veterans perceived people to be threatening, untrustworthy betrayers (p. 270). Conflicts with intimacy included relationships with parents and people the veterans formerly trusted prior to the war (p. 269).
I initially became interested in studying vulnerability after observing combat veterans with PTSD keeping their backs against a wall at all times. This was usually near a doorway. I surveyed scores of veterans concerning what they felt or experienced while positioning themselves like this. Without exception, they reported or agreed to feeling vulnerable and/or easily hurt. They denied feeling anxious or afraid. Because this behavior was so characteristic of combat veterans with PTSD, the experience of vulnerability had to be important to that condition.
The GVS includes the following thematic ideas: Trust/mistrust, including of family members, fear of intimacy and rejection, anxiety, feeling vulnerable, physically threatened, indecisive, discomfort in new situations, sensitivity to criticism, social anxiety, feeling emotionally distant and alienated from others, expecting others to take advantage, feeling/believing others stare and/or talk about them, and fears others will retaliate against them.
The severity of feeling vulnerable may be mild, moderate, or severe, based on the persistence and intensity of symptoms. Individuals with milder forms of vulnerability may actively seek out alliances and relationships with people or organizations who are perceived to be powerful and protective. People with a moderate degree of vulnerability may repeatedly seek out relationships and then push them away once they become fearful of intimacy. People with a severe degree of vulnerability may choose to isolate themselves from all meaningful relationships, even if they feel lonely for companionship.
It is important to note that the GVS was constructed while I treated Vietnam combat veterans with PTSD who reported significant symptoms of emotional numbing. I believe that numbing protects and prevents a person from feeling embarrassed or ashamed. I learned from clinical experience that embarrassment and shame are important symptoms associated with the syndrome of vulnerability in people who are not numb.
How is the experience of anxiety associated with vulnerability different from the experience of anxiety associated with Generalized Anxiety Disorder (GAD)? Diagnostic criteria for GAD includes anxiety, worry, impaired concentration and memory, sleep impairment, muscle tension and irritability. Difficulties with social interactions and social functioning are entirely secondary to the intensity of anxiety symptoms enumerated above.
In contrast, problems with vulnerability primarily focus on difficulties a person experiences with regard to relating to other people and becoming fearful of environmental threats. A person who feels vulnerable is acutely aware of being easily hurt by what others might say or do, or any potential threat within the environment.
It is of interest that both natural and man-made disasters can induce symptoms of PTSD and vulnerability. Feelings of vulnerabilty can engender mistrust and paranoia, even if unrelated to the actual stressor experience.
Application of the Glover Vulnerability Scale (GNS)©
The GVS is a 21 item self-report scale that measures the frequency of experiences from the previous week. GVS scores were found to significantly distinguish levels of functioning within the population of Vietnam combat veterans diagnosed with PTSD. They also significantly distinguished outpatient male veterans with PTSD from outpatient males diagnosed either with Anxiety Disorder or Major Depressive Disorder. GVS scores demonstrated that the scale was a useful measure for assessing severity of vulnerability within the PTSD population. The GVS scores also showed an ability to distinguish between populations exposed to trauma and populations identified to be either depressed or anxious but not exposed to trauma.
An additional study demonstrated that GVS scores were found to be significantly higher in two inpatient groups of females with histories of trauma suffering from Dissociative Identy Disorder (DID) and Self-Injurious Behavior (SIB) than in a group of in-patient females diagnosed with Major Depressive Disorder (MDD) and a control group of females. Within the female control group, those who reported a history of exposure to trauma scored significantly higher on the GVS than those who did not. Again, this emphasized the salient connection between exposure to trauma and vulnerability.
Combat veterans reported having dreams that illustrated the experience of vulnerability, such as seeing glaring eyes staring at them and being encircled in the night by enemy soldiers or wild predatory animals. People who do not experience numbness, but feel vulnerable, may dream of being embarrassed and ashamed in public, for example, by finding themselves exposed and naked in a public situation.
Numbing does not protect someone from feeling vulnerable. In fact, there was a high positive correlation between scores on the numbing and vulnerability scales. The more numb a person reported feeling positively correlated with the more vulnerable he/she felt.
The exception to this may be individuals who become profoundly numb and lose all sensation, including that of fear or feelings of vulnerability. These people may become sensation-seekers and thrill-seekers.
There are certain mental states that are incompatible with feeling vulnerable, such as mania and rage. Psychopathy, although not listed in the DSM-5 as an independant disorder, would also be incompatible with feeling vulnerable.
The GVS is a 21 item self-report scale that measures the frequency of experiences from the previous week. GVS scores were found to significantly distinguish levels of functioning within the population of Vietnam combat veterans diagnosed with PTSD. They also significantly distinguished outpatient male veterans with PTSD from outpatient males diagnosed either with Anxiety Disorder or Major Depressive Disorder. GVS scores demonstrated that the scale was a useful measure for assessing severity of vulnerability within the PTSD population. The GVS scores also showed an ability to distinguish between populations exposed to trauma and populations identified to be either depressed or anxious but not exposed to trauma.
An additional study demonstrated that GVS scores were found to be significantly higher in two inpatient groups of females with histories of trauma suffering from Dissociative Identy Disorder (DID) and Self-Injurious Behavior (SIB) than in a group of in-patient females diagnosed with Major Depressive Disorder (MDD) and a control group of females. Within the female control group, those who reported a history of exposure to trauma scored significantly higher on the GVS than those who did not. Again, this emphasized the salient connection between exposure to trauma and vulnerability.
Combat veterans reported having dreams that illustrated the experience of vulnerability, such as seeing glaring eyes staring at them and being encircled in the night by enemy soldiers or wild predatory animals. People who do not experience numbness, but feel vulnerable, may dream of being embarrassed and ashamed in public, for example, by finding themselves exposed and naked in a public situation.
Numbing does not protect someone from feeling vulnerable. In fact, there was a high positive correlation between scores on the numbing and vulnerability scales. The more numb a person reported feeling positively correlated with the more vulnerable he/she felt.
The exception to this may be individuals who become profoundly numb and lose all sensation, including that of fear or feelings of vulnerability. These people may become sensation-seekers and thrill-seekers.
There are certain mental states that are incompatible with feeling vulnerable, such as mania and rage. Psychopathy, although not listed in the DSM-5 as an independant disorder, would also be incompatible with feeling vulnerable.
One frequent source of confusion for clinicians regarding
the phenomenon of numbness includes the fact that
patients often mistakenly report symptoms of depression
occurring at the same time as feeling numb.
One frequent source of confusion for clinicians regarding the phenomenon of numbness includes the fact that patients often mistakenly report symptoms of depression occurring at the same time as feeling numb.
The Glover Numbing
and Vulnerability Scales
Answer each question with a number that ranges from 1-7, which indicates
the frequency of the experience this past week:
Answer each question with a number that ranges from 1-7, which indicates the frequency of the experience this past week:
Revised Glover Numbing Scale (GNS)©
Scoring for the GNS©:
Item #s: 1, 4, 6, 8, 13, 14, 16, 18, 19, 21, 22, 24, 25, 26, 30, 31, 33, 35 are reverse scored. The range of possible sum scores for this scale is 35-245.
- 1.I feel love or affection for others
- 2.I lose track of time
- 3.I act mechanically like a robot
- 4.I feel in touch with who I am
- 5.My body feels sluggish or heavy
- 6.My vision is clear
- 7.My body feels numb
- 8.I feel full of life
- 9.Nothing matters or means anything to me
- 10.My thoughts are slowed down
- 11.I feel pins and needles in my body
-
12.I feel emotionally numb, hollow, dead, shut down (circle one or more
of the adjectives that apply) - 13.I care about my friends
- 14.I am interested in outside activities (for example, hobbies, sports, etc)
- 15.I pretend I have feelings when I really don’t
- 16.My thinking is clear
- 17.I feel empty – no feelings inside
- 18.I have a normal sex drive
- 19.When I get angry, I care who might get hurt
- 20.Others tell me I look upset, or angry, or sad – and I don’t know what they are talking about
- 21.I feel motivated to do things
- 22.I am aware of my behaviors
- 23.My body feels paralyzed
- 24.I am optimistic
- 25.I feel connected with other people
- 26.I retain information
- 27.When I get angry I feel destructive
- 28.I feel that I am in a fog
- 29.I think about revenge and getting even
- 30.My memory is adequate for every day things
- 31.I care about myself
- 32.A wall exists between me and other people
- 33.I enjoy laughing
- 34.My mind goes blank
- 35.I am able to pay attention
Glover Vulnerability Scale (GVS)©
Scoring for the GVS©:
Item #s: 1, 4, 6, 7, 9, 10, 11, 12, 14, 17, 18, 20, 21 are reverse scored. The range of possible sum scores for this scale is 21-147.
- 1.I trust people
- 2.I leave people or push them away before they can get too close
- 3.I feel vulnerable and/or physically threatened
- 4.I feel calm and relaxed
-
5.I am afraid that if I allow myself to get too close to other people
they might reject me - 6.I feel comfortable in new places and situations
- 7.I trust my family
- 8.People stare at me
- 9.I feel accepted by people
- 10.I take criticism easily
- 11.I am comfortable having conversations with people
- 12.I feel a close bond with my family
- 13.People talk about me
- 14.I feel comfortable opening up to other people
- 15.I worry that people might retaliate against me
- 16.I am distant and alienated from people
- 17.I feel friendly towards people
- 18.I find it easy to make decisions
- 19.I expect people to take advantage of me
-
20.I feel comfortable being in a crowded place (for example,
a movie theatre, restaurant, shopping mall, etc.) - 21.I enjoy socializing with friends
- 1.I trust people
- 2.I leave people or push them away before they can get too close
- 3.I feel vulnerable and/or physically threatened
- 4.I feel calm and relaxed
-
5.I am afraid that if I allow myself to get too close to other people
they might reject me - 6.I feel comfortable in new places and situations
- 7.I trust my family
- 8.People stare at me
- 9.I feel accepted by people
- 10.I take criticism easily
- 11.I am comfortable having conversations with people
- 12.I feel a close bond with my family
- 13.People talk about me
- 14.I feel comfortable opening up to other people
- 15.I worry that people might retaliate against me
- 16.I am distant and alienated from people
- 17.I feel friendly towards people
- 18.I find it easy to make decisions
- 19.I expect people to take advantage of me
- 20.I feel comfortable being in a crowded place (for example, a movie theatre, restaurant, shopping mall, etc.)
- 21.I enjoy socializing with friends
The GVS may be reproduced for free for U.S. governmental purposes. Development and validation studies of the Glover Vulnerability Scale are described in “Vulnerability Scale: A Preliminary Report of Psychometric Properties.” Psychological Reports 75, 1651-1668. Glover, H., Ohlde. C. Silver, S., Packard, P., Goodnick, P., and Hamlin, C. The Revised Glover Numbing Scale was copywritten in 2019.
The GVS may be reproduced for free for U.S. governmental purposes. Development and validation studies of the Glover Vulnerability Scale are described in “Vulnerability Scale: A Preliminary Report of Psychometric Properties.” Psychological Reports 75, 1651-1668. Glover, H., Ohlde. C. Silver, S., Packard, P., Goodnick, P., and Hamlin, C. The Revised Glover Numbing Scale was copywritten in 2019.
Reverse Scoring Key For The GVS & GNS:
1
7
2
6
3
5
4
4
5
3
6
2
7
1
Publications
Enning, F., Schmahl, C. (2022).
“Treatment of dissociative sympstoms with nalmefene in patients with borderline personality disorder and complex posttraumatic stress disorder.” Der Nervenarzt Volume 93, pages 503-505, (2022).
Ramirez, S.M., Glover, H.,Ohlde, C., Mercer, R., Goodnick, P. Hamlin, C., and Perez-Rivera, M.J. (2001).
“Relationship of Numbing to Alexithymia, Apathy, and Depression.” Psychological Reports 88: 189-200.
Glover, H., Lader, W., Walker-O’Keefe, J., and Goodnick, P. (1997).
Glover, H. (1997).
Glover, H. (1996).
“Critique of Fluoxetine study in PTSD.” Journal of Clinical Psychiatry 57: 373-374.
Glover, H., Ohlde, C., Silver, S., Packard, P., Goodnick, P., and Hamlin, C. (1994).
“Vulnerability Scale: a preliminary report of psychometric properties.” Psychological Reports 75: 1651-1668.
Glover, H. (1995).
Glover, H., Ohlde, C., Silver, S., Packard, P., Goodnick, P., and Hamlin, C. (1994).
“Vulnerability Scale: a preliminary report of psychometric properties.” Psychological Reports 75: 1651-1668.
Glover, H., Ohlde, C., Silver, S., Packard, P., Goodnick, P., and Hamlin, C. (1994).
“Numbing Scale: Psychometric properties, a preliminary report.” Anxiety 1: 70-79
Glover, H. (1993)
“A preliminary trial of nalmefene for the treatment of emotional numbing in combat veterans with post-traumatic stress disorder.“ Israel Journal of Psychiatry 30: 255-263.
Glover, H. (1992).
“Emotional numbing: A possible endorphin mediated phenomenon associated with post-traumatic stress disorders and other allied psychopathologic states.” Journal of Traumatic Stress 5: 643-675.
Glover, H., Pelesky, C.A., Bruno, R., Sette, R. (1990).
“Post-traumatic stress disorder conflicts in Vietnam combat veterans: a confirmatory factor analytic study.” Journal of Traumatic Stress 3: 573-591.
Glover, H. (1988).
“Four Syndromes of post-traumatic stress disorder: Stressors and conflicts of the traumatized with special focus on the Vietnam combat veteran.” Journal of Traumatic Stress 1: 57-78.
Glover, H. (1985).
“Guilt and aggression in Vietnam veterans.” American Journal of Social Psychiatry 1: 15-18.
Glover, H. (1984).
“Themes of mistrust and the posttraumatic stress disorder in Vietnam veterans” American Journal of Psychotherapy 37: 445-452
Glover, H. (1984).
“Survival Guilt and the Vietnam Veteran.” Journal of Nervous and Mental Disease 172: 393-397.